Vertical Implant Positioning: Every Connection Has Its Correct Depth
In brief — An implant inserted at the wrong depth relative to its connection type violates the biological width or exposes surfaces meant to remain submerged. Bone-level and tissue-level implants do not get positioned the same way. Conical connections, through cold welding, change the rules — but only with precision-manufactured components. This article explains why, with a visual that makes the concept immediately clear.
Sintesi (IT) — Un impianto inserito alla profondità sbagliata rispetto al tipo di connessione viola lo spazio biologico o espone superfici che dovrebbero restare sommerse. Bone-level e tissue-level non si posizionano allo stesso modo. La connessione conica, grazie alla fusione a freddo, cambia le regole — ma solo se la componentistica è precisa. Questo articolo spiega perché, con una grafica che chiarisce il concetto in un colpo d’occhio.
Implant positioning is often discussed in terms of angulation, distance from adjacent teeth, or bucco-lingual position. The vertical dimension — how deep — receives less attention than it deserves. Yet depth determines where the microgap sits relative to the bony crest, and the microgap is the critical point from which resorption starts — or does not start.
I have addressed this in a previous article on avoidable horrors in implantology. Here I want to isolate a single concept and make it visually unambiguous: every implant connection type has a correct placement depth, and confusing them is a biological error.
The Implant Connection Must Sit Where It Was Designed to Sit
Every implant system positions the implant-abutment interface at a precise level relative to the bony crest. This engineering choice is not arbitrary — it is the mechanical translation of a biological principle: if you bring a reservoir of microorganisms deep into the tissues, those microorganisms will have negative effects on the surrounding structures.
When the implant is placed deeper than its design dictates, the connection ends up at a level that is damaging to surrounding tissues. The chronic inflammatory infiltrate that establishes itself at the connection microgap directly attacks the marginal bone. The result is early, predictable resorption.
Conversely, if the implant is too shallow relative to its design, the transmucosal portion or machined collar remains exposed above the gingiva, compromising aesthetics. The rough implant surface must always remain subcrestal.
Bone-Level: at the Crest, Neither Above Nor Below
Bone-level implants are designed to be placed with their platform at the crestal bone level. All transmucosal management is delegated to the abutment — it is the abutment that crosses the mucosa, not the implant.
The advantage is versatility: the abutment most suitable for the patient’s biotype and the type of restoration can be freely selected. But the price is precision in vertical positioning. If a bone-level implant with an external or flat-to-flat connection goes too deep, the microgap drops to an unfavorable level and resorption is inevitable.
If it is too shallow, the rough implant surface remains above the bony crest, where it will favor the establishment of aggressive biofilm and peri-implantitis. Aesthetics — especially in the anterior sector — suffers severely.
Lachmann et al. (2006) demonstrated in Clinical Oral Implants Research that subcrestally placement of just 1.5 mm in bone-level implants with non-conical connections can cause significantly greater bone resorption compared to juxta-crestal positioning.
The Exception That Changes Everything: the Conical Connection
Everything stated above applies — strictly — to external connections, flat-to-flat designs, and internal hexagons. It applies to every interface where any space exists between implant and abutment, however microscopic, that bacteria can colonize.
The conical connection changes the rules.
In a well-designed taper coupling manufactured to tight tolerances, something different happens: the two titanium pieces lock together with such friction that they achieve intimate, near-molecular contact. Metallurgists call this cold welding. This is not a metaphor: Scarano et al. (2016) in Implant Dentistry, using 3D X-ray microtomography, demonstrated that in Morse taper connections (5° total / 2.5° per side), no detectable separation exists at the conical interface — absolute congruence, no microgap. Internal hexagonal and trilobate connections, in the same study, showed numerous voids and discontinuities.
This has enormous biological consequences. If the microgap virtually does not exist, there is no percolation. No percolation means no infiltration of microorganisms or microbial products. Without a chronic bacterial infiltrate at the interface, bone has no reason to resorb — even when the implant is positioned at or below the crest.
D’Ercole et al. (2022) in Bioengineering quantified this by inoculating bacteria into the connections of 60 implants: bacterial contamination occurred in 45% of external hexagonal connections, 55% of internal hexagonal connections, and only 20% of Morse taper connections. The seal is not perfect in an absolute sense — no mechanical system is — but the difference is decidedly significant.
This is why bone-level implants with a conical connection and intrinsic platform switching can be placed at juxta-crestal or even slightly subcrestally depth without paying the biological price that other connections impose. Camps-Font et al. demonstrated in a network meta-analysis that internal conical connections produce significantly less marginal bone loss than external or internal flat connections at 12 months after prosthetic loading.
Linkevičius’s 4 mm rule for mucosal thickness and vertical implant positioning works precisely because, with a hermetic connection, subcrestally positioning does not equal a sentence of resorption.
But — and this must be stated clearly — cold welding depends on manufacturing precision. A Morse taper with loose tolerances, or with non-original components, loses its purpose. Imprecise, modified, or third-party components turn a conical connection into a leaking connection. A connection fabricated by casting a calcinable abutment is an abomination in this context. Moreover, an imprecise conical connection exposes the implant to a real fracture risk.
I have addressed this extensively in Avoidable Horrors, with evidence from Caricasulo, Camps-Font, and the review by Laleman and Lambert. The direction is unambiguous: internal conical connections, when well-manufactured and with platform switching, offer biological sealing that other connections cannot approach.
Tissue-Level: the Machined Collar Must Emerge, Always
Tissue-level implants have a machined collar designed to traverse the mucosa. The microgap is shifted above the crest, at soft tissue level — away from bone. This is their entire rationale.
But if a tissue-level is placed too deep — as though it were a bone-level — the machined collar ends up in bone. And the machined collar is not designed for osseointegration: it is smooth, not osteophilic. The result is a zone of biomechanical weakness.
But that is not the real problem. After all, smooth implants (the classic Swedish designs) integrated for decades.
The concrete and serious problem is that biological width invasion triggers resorption starting from the connection. The biological space re-establishes itself from that level outward.
This is the most common and most serious error I see in clinical practice: tissue-level implants sunk like bone-levels, and the clinician wonders why the bone recedes. Or, alternatively, they check at time zero: “All good! See you later.” Often with immediate loading as well.
And when tissue-level implants are inserted below the bone level, the site is condemned to severe 360° resorption around the connection extending 3–3.5 mm in depth (Berglundh & Lindhe, 1996). What is the rationale for such a choice?
Astrand et al. (2004) in Clinical Implant Dentistry and Related Research had already compared placements at different depths in Brånemark implants (external hexagonal connection), documenting that marginal bone resorption is directly correlated with the vertical position of the interface relative to the crest.
Platform Switching: an Added Tolerance, Not Insurance
Connections with platform switching — where the abutment diameter is smaller than the implant platform — shift the inflammatory infiltrate toward the implant center and away from the marginal bone. This confers a degree of tolerance for slightly subcrestally positioning.
Canullo et al. (2010) in Clinical Oral Implants Research demonstrated that platform switching reduces marginal bone resorption compared to platform-matching connections. But it is not a pass to position implants at arbitrary depths. The biological principle holds: the microgap has an ideal position, and every deviation has a cost.
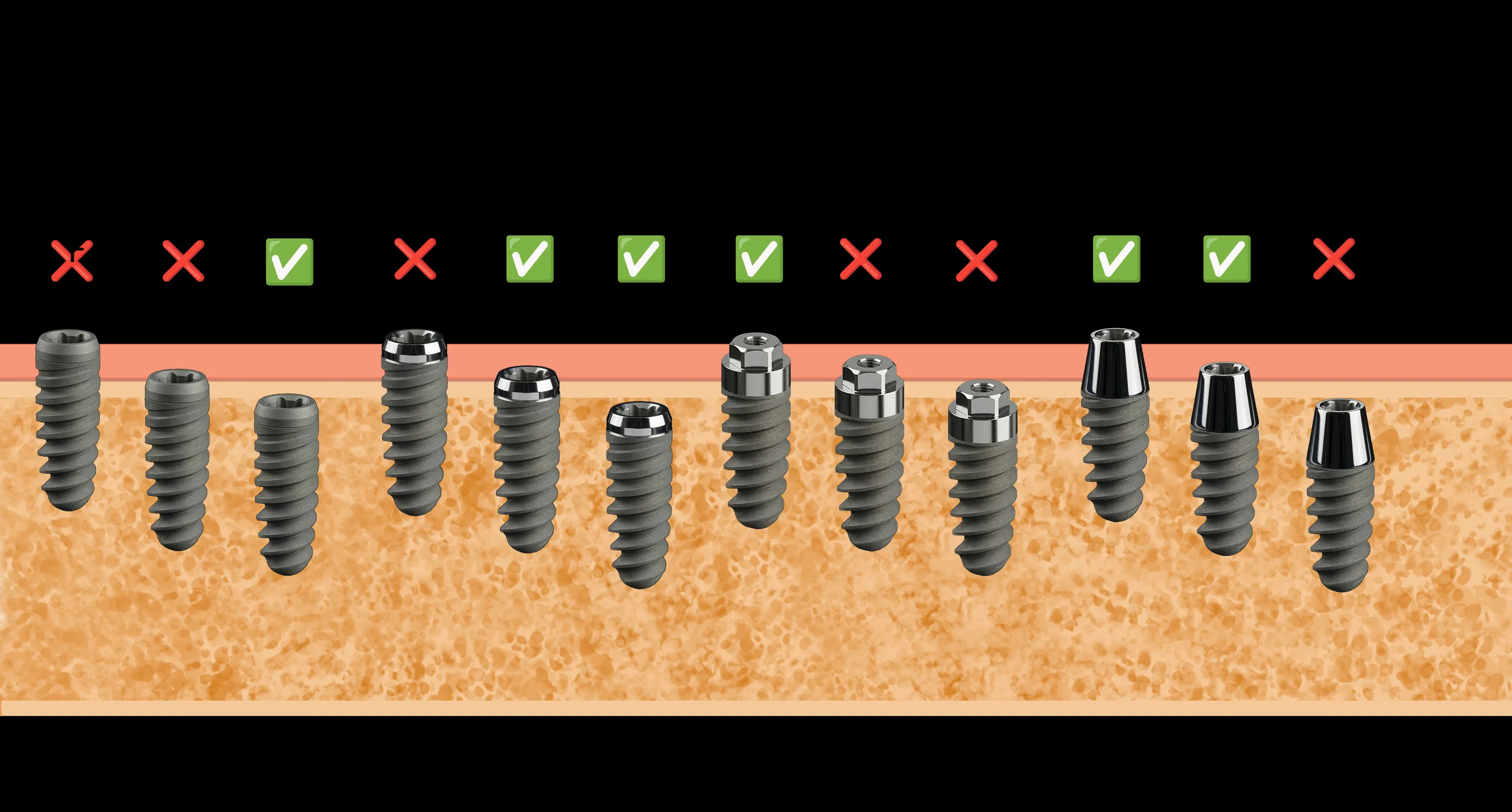
The Visual: Reading Positioning at a Glance
The image accompanying this article shows different implants with different connections positioned in the mucosa and bone. Green checks indicate correct positioning for that specific connection type. Red Xs indicate errors — too deep, too shallow, or simply the wrong type of depth for that connection.
There is no “universally correct” depth. There is the correct depth for that implant type and that connection. Confusing the two is like laying a building’s foundation at the wrong floor: the structure holds — for a while.
What Changes in Practice
The clinical implications are concrete:
-
Know your system: before placing an implant, the clinician must know exactly where the manufacturer has positioned the microgap and what the recommended placement depth is. This is not a detail — it is the design specification.
-
Use guided surgery: digital planning and surgical guides do not only serve to avoid the inferior alveolar nerve. They position the implant at the correct depth with precision that freehand technique cannot consistently guarantee.
-
Do not mix philosophies: a tissue-level is not a bone-level with a machined collar. They are two different biological concepts, and placing them identically is a conceptual error before a technical one. I have discussed this in relation to the biomechanical consequences of malpositioning.
-
Abutment height matters: Galindo-Moreno et al. (2014) in Journal of Dental Research demonstrated that abutments shorter than 2 mm favor bone resorption. Implant depth and abutment height are two sides of the same coin — bone responds to both.
Frequently Asked Questions
What is the difference between a bone-level and a tissue-level implant? The bone-level has its platform at crestal bone level and delegates transmucosal management to the abutment. The tissue-level has an integrated machined collar that crosses the mucosa, shifting the microgap away from bone. Two different philosophies requiring different placement depths.
What happens if an implant is placed too deep? The microgap drops below the crestal bone. The inflammatory infiltrate at that level attacks the marginal bone, causing progressive resorption. In tissue-level implants, the machined collar ends up in bone — a zone of mechanical and biological weakness.
Does a conical connection eliminate the microgap problem? It drastically reduces it. The taper coupling creates a cold weld between the two titanium pieces that eliminates, or nearly eliminates, bacterial percolation. This is why bone-level implants with a conical connection tolerate subcrestally positioning. But the seal depends on manufacturing precision: imprecise or non-original components cancel the advantage.
Does platform switching solve the depth problem? It mitigates it, does not solve it. Platform switching shifts the inflammatory infiltrate toward the implant center, reducing marginal resorption. Combined with a conical connection, it offers maximum protection of marginal bone. No design is a pass for arbitrary positioning.
How is depth controlled during surgery? Guided surgery is the most reliable method. In freehand, periodontal probes and intraoperative radiographs are used. The reference point is the bony crest — not the gingiva, which can be misleading.
Why do so many clinicians get the depth wrong? Often because they use different systems without adapting their technique to the specific connection type. Or because they chase primary stability by sinking the implant deeper than necessary. Stability comes from correct site preparation, not from excessive depth.
Is an implant placed too shallow less serious? No, it is a different error. The rough surface exposed above bone favors aggressive biofilm accumulation and peri-implantitis. In tissue-level implants, the endosseous threads may remain uncovered with loss of stability.
References
- Scarano A, Valbonetti L, Degidi M, et al. Implant-Abutment Contact Surfaces and Microgap Measurements of Different Implant Connections Under 3-Dimensional X-Ray Microtomography. Implant Dent. 2016;25(5):656-662. PubMed
- D’Ercole S, Dotta TC, Farani MR, et al. Bacterial Microleakage at the Implant-Abutment Interface: An In Vitro Study. Bioengineering. 2022;9(7):277. PubMed
- Camps-Font O, Martín-Formal G, Mir-Mari J, et al. Fracture resistance, mechanical complications and marginal bone loss in internal conical connection versus external hexagonal implants: Systematic review and network meta-analysis. J Prosthet Dent. 2022. DOI
- Canullo L, Fedele GR, Iannello G, Jepsen S. Platform switching and marginal bone-level alterations: the results of a randomized-controlled trial. Clin Oral Implants Res. 2010;21(1):115-121. PubMed
- Lachmann S, Kimmerle-Müller E, et al. Associations between peri-implant crevicular fluid volume, concentrations of crevicular inflammatory mediators, and composite IL-1A -889 and IL-1B +3954 genotype. Clin Oral Implants Res. 2006;17(1):2-9. PubMed
- Galindo-Moreno P, León-Cano A, Ortega-Oller I, et al. Prosthetic abutment height is a key factor in peri-implant marginal bone loss. J Dent Res. 2014;93(7 Suppl):80S-85S. PubMed
- Berglundh T, Lindhe J. Dimension of the periimplant mucosa. Biological width revisited. J Clin Periodontol. 1996;23(10):971-973. DOI
- Astrand P, Engquist B, Dahlgren S, et al. Astra Tech and Brånemark system implants: a 5-year prospective study of marginal bone reactions. Clin Oral Implants Res. 2004;15(4):413-420. PubMed
FAQ
- What is the difference between a bone-level and a tissue-level implant?
- The bone-level implant has its platform at crestal bone level, delegating transmucosal management to the abutment. The tissue-level has an integrated machined collar that crosses the mucosa, shifting the microgap away from the bone. These are two different philosophies, requiring different placement depths.
- What happens if an implant is placed too deep?
- The microgap drops below the crestal bone. The chronic inflammatory infiltrate that forms at that level attacks the marginal bone, causing progressive resorption. In tissue-level implants, the machined collar ends up in bone — a zone of mechanical and biological weakness.
- Does a conical connection eliminate the microgap problem?
- It drastically reduces it. The taper coupling creates a cold weld between the two titanium pieces that eliminates, or nearly eliminates, bacterial percolation. This is why bone-level implants with a conical connection tolerate subcrestally positioning. But the seal depends on manufacturing precision: imprecise or non-original components cancel out the advantage.
- Does platform switching solve the depth problem?
- It mitigates it, it does not solve it. Platform switching shifts the inflammatory infiltrate toward the implant center, reducing marginal resorption. Combined with a conical connection, it offers maximum protection of marginal bone. But no design is a pass for arbitrary positioning.
- How is depth controlled during surgery?
- Guided surgery is the most reliable method. In freehand placement, periodontal probes and intraoperative radiographs are used. The reference point is the bony crest — not the gingiva, which can be misleading.
- Why do so many clinicians get the depth wrong?
- Often because they use different systems without adapting their technique to the specific connection type. Or because they chase primary stability by sinking the implant deeper than necessary. Stability is achieved with correct site preparation, not with excessive depth.
- Is an implant placed too shallow less serious?
- No, it is a different error. The rough surface exposed above the bone favors aggressive biofilm accumulation and peri-implantitis. In tissue-level implants, the endosseous threads may be left uncovered with loss of stability.
- Where can I learn more about the consequences of malpositioning?
- The biomechanical consequences are covered in a dedicated article, and connection-related issues in Avoidable Horrors: Implants, Connections, and Components.
References
Looking for a specialist?
Implantologia a Frosinone →Impianti dentali, carico immediato e rigenerazione ossea
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment